

Reply To:
Name - Reply Comment
In most of these countries, it had been found out, the current guidance on Coronavirus “largely ignores” the implications for public health and clinical responses of the older people.
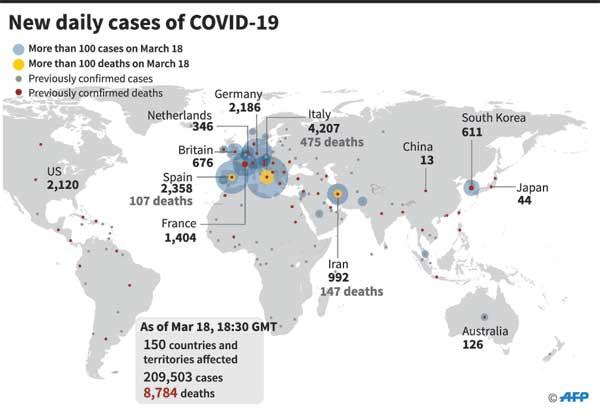
We are living in unheard-of times. According to updates, as of 10:18 am, Mar 18, the COVID-19 pandemic is escalating rapidly with 200,071 confirmed cases and 8,009 deaths in 152 countries.
The majority of cases and deaths are among people aged 60 years and older living in low- and middle-income countries (LMICs) like Sri Lanka, where healthcare resources to treat people and control the epidemic are limited. 
In most of these countries, it had been found out, the current guidance on Coronavirus “largely ignores” the implications for public health and clinical responses of the older people.
Sri Lanka is no exception. We have over 4.6 million people aged 55 years and above. Their health systems are weaker, leaving them vulnerable to the worst impacts of COVID-19. Standard guidance which is more relevant to high-income countries has been produced for older people as well.
Even before the COVID-19 reached 100 countries around the world, early data from China - where the outbreak started - suggested that older adults were the most vulnerable to the worst effects of the disease. Now, that data, along with emerging research from Italy - the second-most-affected country in the world - is showing just how dangerous COVID-19 is for older people, and others with heart, lung, and immunological conditions.
In a late February report, researchers of China’s Centre for Disease Control looked at the first 72,314 patients with confirmed or suspected COVID-19 and discovered a huge variation in the case fatality rate by age group. In short, the disease appears to be deadlier in people with each passing decade.
Age, however, doesn’t tell the whole story about who is at risk of severe disease. Many of these factors are concentrated among older adults, but younger people with certain underlying chronic conditions are also at risk. The lessons we learn from older patients could help us treat and prevent the spread. That makes it all the more important to understand the variables that put older adults at greatest risk so we can develop a strategy to protect society as a whole.
It is common knowledge that as we age, the systems our bodies use to fight disease wear down. Not only does the body will have a harder time fighting off new infections like COVID-19, but it is also more likely to be afflicted by chronic diseases that make the immune system weaker.
Let us see how our bodies get worse at fighting foreign invaders, including viruses like SARS-CoV-2, which causes COVID-19. In older adults, the number of white blood cells that find and help eliminate infections can decline.
The cells also become less adept at identifying new pathogens to fight. In the case of COVID-19, the virus can also damage the immune cells that might otherwise overcome the virus. If there are fewer of these cells, to begin with, and they’re also weaker than they once were, an illness can do more damage. That is what happens in older people.
Writing in the British Medical Journal, researchers from the University of East Anglia (UEA), London School of Hygiene & Tropical Medicine (LSHTM) and Samson Institute for Ageing Research (SIFAR), Cape Town, South Africa request for an age perspective to be included explicitly in national and global planning on COVID-19.
In their editorial, Prof Peter Lloyd-Sherlock of UEA, Prof Shah Ebrahim and Prof Martin McKee of LSHTM, and Dr Leon Geffen at SIFAR note that the largest numbers of deaths will occur among older people in lLMICs. These countries contain 69 per cent of the global population aged 60 and over, and health systems which are less extensive and less focussed on the needs of older people than in high-income countries.
Prof Lloyd-Sherlock says: “The global response to coronavirus must be directed towards those groups who will face the most devastating consequences. So far, this has not happened. We are facing an unprecedented and enormous wave of mortality among older people in these countries.”
They maintain that in LMICs, the risk of infection for older people will be high because living arrangements are often cramped and overcrowded. The researchers suggest social distancing policies must consider the already precarious existence of many older people, particularly those living alone or dependent on others for care and support. These people may face barriers to obtaining food and other essential supplies if quarantine conditions become more widespread.
The researchers add: “The capacity of health systems in LMICs to screen, let alone treat, the virus will be very limited: Even before COVID-19 emerged, older people already faced significant barriers of access to health services and support, including affordability, and age-based discrimination.”
They further comment: “It will not be easy to deal with these problems, especially in settings where there is often weak public health infrastructure, a lack of gerontological expertise at all levels of the health system, and limited trust in government. However, a first step would be to recognise that these problems exist”.
“An age perspective should be included explicitly in the development of national and global planning for COVID-19, and a global expert group on older people should be formed to support with guidance and response to the virus in both residential facilities and home settings.
“As new knowledge emerges, this group can identify and evaluate cost-effective therapies and interventions that respond to the particular needs of older people in LMICs living in challenging settings, where formal health service infrastructure is limited.”
They conclude: “Previously, some of the authors have argued that global health priority setting is institutionally ageist. COVID-19 offers an opportunity to prove us wrong.”
In the absence of clear comprehensive guidelines for prevention and control of COVID-19 among older people, ad hoc policies are emerging. We heard how Italy prioritised for younger when they experienced scarce hospital and intensive care services. Reports also indicate that in the UK, people aged 70 and over will be expected to self-isolate themselves for up to four months in the coming weeks.
In LMICs, older people provide an integral economic and social resource to societies, including bringing up grandchildren to support the labour mobility of their adult children and relatives. Beyond grief and bereavement, the implications of COVID-19 deaths among the older population will be profound.
The ability of health systems to cope with a surge in demand is extremely limited, especially for aged patients needing intensive care. Health systems in LMICs face severe constraints on capacity at normal times and are unlikely to be able to keep up, especially if the precarious staffing levels and limited gerontological expertise are reduced further by illness.
Coming back to Sri Lanka, that means that all of us have to work together to control the spread of COVID-19, and we all stand to suffer if we don’t. Younger people can limit the infection’s spread to the more vulnerable with good hygiene, self-isolating when they are sick, and practising social distancing measures so they can avoid getting the virus and passing it along to their older family members.
This is particularly important for COVID-19 since people can transmit the virus before experiencing any symptoms. And we’re still learning about the dangers of this disease and how quickly it’s spreading, so there may be other groups at risk that we don’t yet understand.


















