21 Feb 2020 - {{hitsCtrl.values.hits}}
 According to the Johns Hopkins University novel-Coronavirus 2019 (COVID-19) tracking map, as many as 64,422 cases have been reported from around the world. While the death toll is spiking every day, it’s important that people take maximum precautions to avoid contact with any sort of contamination. When taking a look at the Sri Lankan situation a multidisciplinary approach was taken to ensure that the Sri Lankan contingent from Wuhan was quarantined and released. At the onset of its outbreak local authorities took maximum precautions to screen visitors from high risk countries. However, pulmonologists believe that this momentum needs to continue and certain facilities need to be upgraded in order to be ready for any further respiratory epidemic.
According to the Johns Hopkins University novel-Coronavirus 2019 (COVID-19) tracking map, as many as 64,422 cases have been reported from around the world. While the death toll is spiking every day, it’s important that people take maximum precautions to avoid contact with any sort of contamination. When taking a look at the Sri Lankan situation a multidisciplinary approach was taken to ensure that the Sri Lankan contingent from Wuhan was quarantined and released. At the onset of its outbreak local authorities took maximum precautions to screen visitors from high risk countries. However, pulmonologists believe that this momentum needs to continue and certain facilities need to be upgraded in order to be ready for any further respiratory epidemic.
What is Coronavirus ?
“Corona means crown and in a sense the virus depicts the shape of a crown,” explained Dr. Neranjan Dissanayake, Consultant Respiratory Physician, Teaching Hospital and District Chest Clinic, Ratnapura. “It has four subspecies alpha, beta, gamma and delta where alpha and beta affect mammals while gamma and delta affects birds as well as mammals. Till 2002 only four Coronaviruses were identified which caused mild upper respiratory tract symptoms including nasal congestion and rhinorrhea and it didn’t show much symptoms in immunocompetent people. However there were severe symptoms in immunocompromised people. However, in 2002 the picture changed with the SARS epidemic – another Coronavirus where over 8000 people were infected and 800 of them died. In 2012 MERs virus outbreak had 30% fatalities where 2400 people developed the condition and 800 died. From a mild neglected virus called corona we see that two epidemics spread throughout the world,” said Dr.Dissanayake.
Explaining its complexities further, Dr. Dissanayake said that the Coronavirus is an RNA virus and has a high amount of ribonucleic acid. “Therefore it has a high mutation rate and can develop into new viruses combining with other DNA material which were not previously seen in the human body. This would cause a significant amount of morbidity and mortality. The protein component has certain areas which facilitates the virus to enter the cell. Usually a virus enter the human body through a receptor while a bacterial infection enter the body through a breach of the immune system or a physical barrier. But viruses use our own proteins to enter our body and cause diseases. Many viruses change their capsule and its difficult to keep track of them thereafter as they appear to be different due to high mutation rate,” he said.
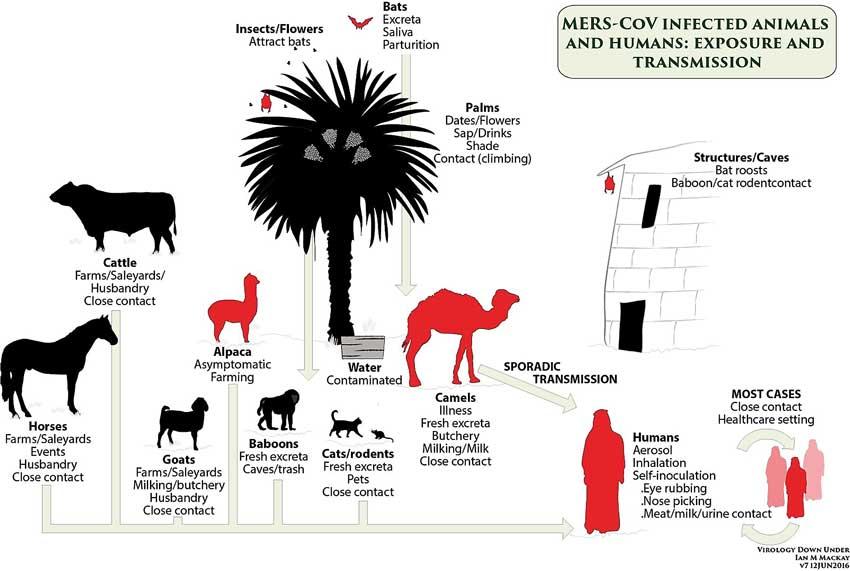
Keep a close watch on bats
He further said that coronaviruses are very common in bats. “A study done in Wuhan has identified different types of Coronaviruses which together can cause the SARS virus,” he added. “Usually these viruses develop in bats or rodents. Then there are intermediary hosts such as civet cats, camels etc. In Sri Lanka we have a lot of bat enclaves and probably they too are harboring the Coronavirus in them. Sometimes we may have a high risk of developing novel Coronavirus ourselves. So we should get the Department of Wildlife Conservation (DWC), virologists, medicinal institutes and it’s time to start surveillance in our bats to see if we have a risk of developing novel Coronavirus,” added Dissanayake.
Common symptoms and minimising risks
According to him fever, breathing difficulty and cough are common symptoms. “In a 41 people study published in January, 40 of them had fever and it’s a good clinical marker that we can use to identify patients with coronavirus apart from cough and myalgia (body pain). We can screen people coming from high risk areas. But they may take paracetamol on their way or if they don’t want to expose themselves they may deliberately reduce fever themselves. So there has to be a mechanism to identify them before they board the plane. Maybe they could be asked to fill a form to see if they have taken paracetamol or if they had fever during the past two-three hours. This way we could prevent other respiratory diseases which can propagate very rapidly in the Sri Lankan context as well. The next one could be influenza or multi-drug resistant tuberculosis which is prevalent in China and India. A major discovery is the reduction of lymphocytes. Chest X-rays of a certain group of people have shown white shadows. When the virus damage the cells there will be inflammation and cause increasing amount of inflammatory cells and fluid to leak into alveoli and eventually the alveoli will be flooded with fluid. When the alveolus is involved the oxygen doesn’t flow from the alveolus into the blood and patient will become hypoxic later,” he explained.
Managing symptoms and complications
Another study analyses 38 people who were critically ill had fever and dyspnea which has been helpful to check patients who need ICU care. Complications showed shock while five of them shad acute cardiac injury. “Apart from that, arrhythmia, acute respiratory distress syndrome and kidney injury had been the main stay of focus. Most patients with dyspnea and hypoxia need ICU care facilities which have respiratory preventive methods installed there. In SL we don’t have such intensive care facilities and therefore about 7% of TB patients die. This is because we don’t have ICU facilities with infective protective measures to manage these patients. Therefore I suggest that we have at least four to five beds in every district general hospital which are significantly covered or protected with quarantine methods to manage patients with infective respiratory diseases. We can identify certain provincial general hospitals for this purpose and can use it to manage other diseases as well. These patients also need high flow oxygen facilities which will reduce burden to the ICU. Another method is Extra Corporeal Membrane Oxygenation (ECMO) that would provide prolonged cardiac and respiratory support to people whose heart and lungs are unable to provide an adequate amount of gas exchange. A the moment have this facility only in Karapitiya,” the doctor said.
Improving facilities
Studies have shown that out of 138 patients about 41% have been infected in hospitals. “A recent case featured one patient with abdominal pain having given the disease to 10 others because he wasn’t diagnosed as having nCoV 2019. We therefore need to appreciate the service by healthcare workers in IDH. Nobody backed out or asked for incentives. They only requested for protective gear only. Everybody from the junior staff to the Consultant has to be protected. We need to get the microbiologists, virologists, respiratory physicians, intencivists, Ministry of Health, armed forces and the veterinary people together, so that we have a huge ball that cannot be penetrated with any other infections,” the doctor said.
21 Dec 2024 4 hours ago
21 Dec 2024 21 Dec 2024
21 Dec 2024 21 Dec 2024
21 Dec 2024 21 Dec 2024
21 Dec 2024 21 Dec 2024





