13 Jan 2017 - {{hitsCtrl.values.hits}}
By Vinuri Weerawardena
The 2016 outbreak of the Zika virus brought the neurological condition Microcephaly to global attention as a significant number of infants whose mothers had contracted the Zika virus were diagnosed with the condition. However, Microcephaly is a condition on its own, even though it has been mainly associated with the Zika virus in the recent past. Microcephaly still remains a major concern worldwide and spreading awareness on its causes, symptoms, prevention and supportive care is of utmost importance.

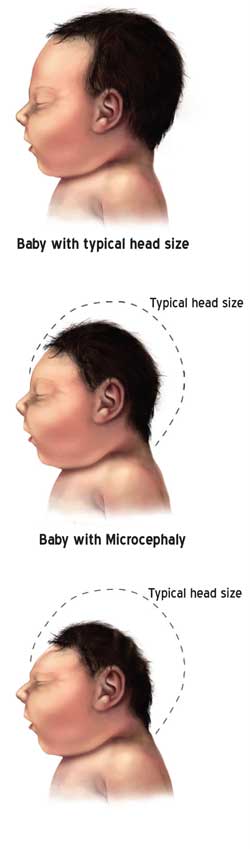
Microcephaly (my-kroh-SEF-uh-lee) is considered a rare neurological condition in which an infant’s head is significantly smaller than the heads of other children of the same age and sex, based on standardized charts. This is usually due to the brain developing abnormally in the womb or not growing as it is supposed to. Microcephaly is often associated with below average mental and cognitive development. This could be congenital or acquired. Many countries including Sri Lanka have no valid data on microcephaly and its causality. Even estimated incidence of microcephaly have wide variation due to the differences in the definition and subjects under study.
The Daily Mirror approached Dr. Kapila Jayarathne, Consultant Community Physician and National Programme Manager- Maternal & Child Morbidity and Mortality Surveillance (Family Health Bureau- MOH) to determine the details of the disease and its presence in the country. He acknowledged the lack of reliable information regarding the incidence of Microcephaly in Sri Lanka. He went onto say that this neurodevelopmental defect came into light in Sri Lanka with the incidence of the Zika virus and public awareness of its effects during this period. As of now, the Family Health Bureau has established a surveillance system to monitor the incidence of Microcephaly cases. Dr. Jayarathne is pleased to report that there are many prospective studies and collaborations awaiting in the year 2017 that will venture into the study of Microcephaly. One such prospective study will be a series of Microcephaly case studies that will inspect every aspect of the defect, its causes and any unique attributes for Sri Lankans.
Meanwhile, it is always safe to be equipped with the necessary knowledge and facts about Microcephaly in order to help family, friends and yourself.

There are several potential causes of Microcephaly, however as in most neurological conditions, the specific cause varies from individual to individual but often the cause remains unknown.
The common causes of Microcephaly as identified by Neurologists are; Infections during pregnancy: toxoplasmosis (caused by a parasite found in undercooked meat), rubella, herpes, syphilis, cytomegalovirus, HIV and Zika viruses. Exposure to toxic chemicals: Maternal exposure to heavy metals like arsenic and mercury, alcohol, radiation, and smoking. Pre- and perinatal injuries to the developing brain: Hypoxia-ischemia, trauma); Genetic chromosomal abnormalities: Down syndrome, Seckel Syndrome. Malnutrition: Severe malnutrition during fetal life. Craniosynostosis: The premature fusing of the joints (sutures) between the bony plates that form an infant’s skull keeps the brain from growing. Treating craniosynostosis (kray-nee-o-sin-os-TOE-sis) usually means the infant needs surgery to separate the fused bones. If there are no underlying problems in the brain, this surgery allows the brain adequate space to grow and develop. Chromosomal abnormalities: Down syndrome and other conditions may result in microcephaly. Decreased oxygen to the fetal brain (cerebral anoxia): Certain complications of pregnancy or delivery can impair oxygen delivery to the fetal brain.
Life expectancy is usually reduced along with poor brain function in children and adults. However this outcome varies based on the presence of associated conditions. Typically life expectancy is low, limited to about 20 years of age, although this depends on the incidence of the aforementioned related abnormalities.
How well a child copes depends on what caused the brain to stop growing, causing the condition. Children with a mild form of this disorder may not have any significant problems. They will grow normally during childhood and adolescence and meet age-appropriate growth milestones as they get older.
Others with more severe Microcephaly will have problems learning and moving. They are more likely to have other medical problems, such as cerebral palsy and epilepsy.
Pre-natal health is of utmost importance when it comes to tackling the prevention of Microcephaly caused by non-genetic factors, i.e. Acquired Microcephaly.
Following are a few general guidelines covering basic maternity health concerns. Following the guidelines could reduce the probability of your child being born with acquired microcephaly. Make a healthy diet part of your lifestyle and take prenatal vitamins. Refrain from the consumption of alcohol and the use of drugs. Stay away from chemicals. Maintain cleanliness, wash hands often and get treatment for any illness as soon as you feel sick. If you have pets, make sure to have someone else change the litter box. Animal feces can spread the parasite that causes toxoplasmosis. Use mosquito repellent when in wooded areas or countries known for mosquitoes. The CDC (Centres for Disease Control and Prevention- USA) says insect repellent is safe to use while pregnant.
Microcephaly can be diagnosed during pregnancy or after the baby is born.
During the pregnancy, diagnosis may be done via means of an ultrasound (which creates pictures of the body). For clear detection during pregnancy, it is advisable to do so through an ultrasound test done in the late 2nd Trimester or early 3rd Trimester.
After the birth of the child, diagnosis would be done by a medical practitioner. A head CT scan or an MRI along with blood tests will help determine whether or not Microcephaly has been detected in the child.
Microcephaly is a life-long condition and may also be life-threatening in some cases. As reiterated throughout the article, it again depends on the severity of this neurodevelopmental condition.
Unfortunately at present, there is no known treatment to ensure that the growth of the head is set on track. However, medical professionals may treat associated conditions and complications arising from microcephaly.
This kind of treatment will focus on managing the child’s condition. Early childhood developmental intervention programmes that include speech, physical and occupational (for development of motor skills) therapies are advised in order ensure the child abilities are strengthened in order to maximize their developmental and intellectual capabilities. Medical practitioners may also recommend medication to control certain complications of Microcephaly such as seizures and hyperactivity.
Early detection is always important when it comes to neurodevelopmental conditions, as such detection will enable parents addressing the condition earlier to provide supportive care in order to ensure a comfortable lifestyle for the child.
The primary sign of Microcephaly is the child’s head circumference being significantly smaller than that of other children of the same sex and age. This comparison can be made with the use of standardized growth charts using standardized growth charts. This measurement is compared with other children’s measurements in percentiles. The Sri Lankan growth standards to be used can be found at the WHO site https://www.unicef.org/srilanka/ECDS_report_new%283%29.pdf
Other basic symptoms that can be observed and identified include:
·Poor appetite/feeding
·Unusually high-pitched crying
·Spasticity (involuntary muscle contractions)
If the brain stem of the child has been affected, the condition could be more serious because it is the brain that controls vital survival functions such as respiration.
Therefore, depending on the severity and/or complications of Microcephaly, other symptoms include: Impaired cognitive development, delayed motor functions and speech, facial distortions, dwarfism or short stature, hyperactivity, seizures, difficulties with coordination and balance and other brain or neurological abnormalities.
25 Dec 2024 11 minute ago
25 Dec 2024 17 minute ago
25 Dec 2024 27 minute ago
25 Dec 2024 1 hours ago
25 Dec 2024 3 hours ago





