07 Sep 2018 - {{hitsCtrl.values.hits}}
 It is not uncommon to observe heart attacks in relatively young diabetic patients in our country. By young the author implies those who are less than 60 years of age. Some of them are company executives while the others are professionals and include even doctors. These patients are in the prime of their lives and are supporting young families. What should be noted is that they have reached the top in their professions.The intention of this article is to discuss some preventive aspects of diabetic heart disease (DHD) which hopefully may prevent at least some of these deaths. There is a common saying which goes, “Within every patient having diabetes the enemy of heart disease is hiding”.
It is not uncommon to observe heart attacks in relatively young diabetic patients in our country. By young the author implies those who are less than 60 years of age. Some of them are company executives while the others are professionals and include even doctors. These patients are in the prime of their lives and are supporting young families. What should be noted is that they have reached the top in their professions.The intention of this article is to discuss some preventive aspects of diabetic heart disease (DHD) which hopefully may prevent at least some of these deaths. There is a common saying which goes, “Within every patient having diabetes the enemy of heart disease is hiding”.
This problem may worsen in the future in countries such as Sri Lanka where the incidence of diabetes is rising rapidly. In contrast in more developed countries such as the USA, despite a rise in incidence of diabetes, the death rate is decreasing. This could be attributed to several factors such as the availability of modern treatment techniques as well as the knowledge patents possess about DHD. Even in Sri Lanka these facilities are available to those living in major cities such as Colombo (both in the state and private sectors) and in the state sector in Kandy, Jaffna and Kurunegala.
What is a heart attack?
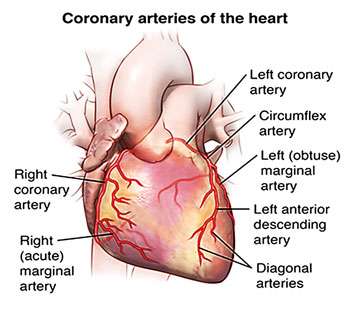
A heart attack occurs when the blood supply to the heart is suddenly blocked by the formation of a blood clot in a blood vessel (coronary arteries) consisting of cholesterol deposits.The clot is formed by platelets, clotting factors present in the blood as well as white blood cells.There are three large coronary arteries supplying the heart muscle with the left coronary being the most important. The next is the anterior descending artery and last is the right coronary artery (please refer to the diagram). A large clot in the left coronary artery would severely affect the area of heart muscle (sometime even death unless unattended) which supplies the chamber (left ventricle) which pushes out almost all the blood to other vital organs such as the brain and the kidneys.
It has been stated that for every patient with diabetes there is another one who remains undiagnosed and therefore could be subjected to heart attacks without even knowing that they ever had diabetes
The deposition of cholesterol does not occur suddenly, but is a life-long process. In fact such cholesterol deposits are found during post-mortems (Sometimes the deceased are very young children) of individuals who pass away due to some other cause. As with diabetes this occurs even in young adults and affects more than one coronary artery (multi vessel disease). Asians, for example Sri Lankans, are known to have such extensive disease regardless whether they live in their motherland or elsewhere.
Why do premature deaths occur?
When patients are young, unless these individuals are treated properly, they succumb to the first attack. This is largely because the additional coronary vessesl given to us by nature, called collaterals, has not opened up. When these vessel are open and even if there is a clot, the blood could be diverted to these vessels there by preventing the death of heart muscle. In contrast it is quite rarely that an elderly person dies of the first attack. This is because given such a patient’s age there has been sufficient time for these collaterals to open up.
What are the factors contributing to the formation of cholesterol deposits in diabetes?
Contrary to popular belief it is not the raised blood sugar alone which contributes to this process. In fact there are other important causes indicated below in the order of importance that contributes to this condition.They are high blood pressure, high cholesterol levels, high blood sugar, presence of protein in the urine, smoking and family history of DHD.
This may explain why some patients, who have very high blood sugar levels, don’t suffer heart attacks since their blood pressure and cholesterol are well under control and the opposite occurs in those who control their sugar level, but do not attend to the two other contributory factors.
Recently it has been shown that certain infections too, such as those of the gums (periodontitis) too could be a contributing factor to this condition.
What really precipitates a heart attack?
What was discussed above was only the causes of deposition of cholesterol in the coronary blood vessels, but the factors that really precipitate the attack is largely unknown.What is known, at least little, is the time of the day. Nearly 70% of the attacks occur in the early hours of the morning, say between 2 am and 7 am. The reason for this is a sudden surge in some hormones such as cortisol and adrenaline. Adrenaline levels could also rise during the other times of the day when there is mental and physical stress (exercise induced heart attacks).
Could low blood sugar (Hypoglycaemia) precipitate a heart attack?
The answer is certainly ‘yes’ and the author has documented several such cases. When the blood sugar drops for whatever the reason, like due to prolonged starvation, the excessive use of anti diabetic drugs and physical exercise, the same hormones come into play. Sometimes such patients die at night during sleep since there is a tendency for the blood sugar to drop since we don’t consume any food during such periods. Some of these heart attacks are ‘silent’ and the patient does not feel any pain. Thus it is mandatory for us to enquire from the patient whether there were symptoms of low blood sugar such as excessive hunger, sweating, dizziness and palpitations before the onset of the attack. It is therefore advisable for diabetic patients to routinely consume a night time snack to prevent low blood sugar at night.
What are the symptoms and signs of a heart attack?
The commonest symptom is of course chest pain which is felt behind the chest bone, throat and even the back. They also could come with sudden loss of consciousness, difficulty in breathing and palpitations. Experienced physicians could even diagnose a heart attack by the way the patient shows where the chest pain is.This is called the ‘Body language’.
The signs (those detected by the Medical officer) include ‘Shock’ where the blood pressure is very low and the pulse impalpable, low or high pulse rate and signs of acute heart failure.
Atypical presentations of a diabetic heart attack
1. A fainting attack which may even go unnoticed both by the patient and the doctor
2. ‘Gastritis’- The label that carries a certain kind of danger. So many lives have been lost due to the low attention paid to this symptom. These patients too complain of chest pain over the front of the chest just like during a heart attack which is named as the so called ‘attribution error’. During such a condition the patient (and some times the doctor) attribute it to the consumption of a hot meal or another type of spicy food.
3. A ‘silent heart attack’ as discussed above is one where there is no pain at all. It has been estimated that nearly 30% of all diabetic patients would manifest such silent heart attacks.This raises the importance of identifying such patients by proper screening methods which would be discussed later.
It should be also stated that sometimes a heart attack could develop gradually where the symptoms discussed above may come on slowly; say for example chest pain which comes on exertion called ‘angina’.
Emergency treatment for a suspected heart attack
1. Emergency treatment should be carried out at home itself no sooner the patient develops the chest pain. A single dose of aspirin (300 mg) should be immediately administered. Studies have shown that early treatment using aspirin would be as effective as administering clot busting medication such as streptokinase. Another type of emergency treatment that could be administered at home is a cocktail of the following drugs.
a.Aspirin 300 mg as indicated above
b.A drug called Clopidogrel =300mg
c. Atorvastain (a cholesterol lowering drug in a dose of 40 mg)
d.Pantaprazole- an acid lowering drug which could prevent the occurrence of gastritis caused by such a high dose of aspirin.
In certain countries this is available as a ‘Heart Pack’ which could be certainly introduced to Sri Lankan homes too.
Tests for a suspected heart attack
1.ECG would be very useful, but in some cases the changes would surface after a few hours only.
2. A blood test called ‘Troponin I’ which too could be positive in a few hours only. Thus the clinical suspicion and all risks associated with suffering a heart attack should be thought of.
3. If the patient is lucky enough to reach a well-equipped hospital a test called ‘angiography’ will be carried out and a piece of hollow metal, called a stent, is introduced immediately. This would by pass the block and restore the blood supply. There are some sophisticated ones called ‘drug eluding’ stents which continue to release drugs given for heart attacks. It is strongly advised that the patient should be transfered to a hospital as soon as possible since timing is very important. Earlier the clot buster medication is given because this would dissolve the clot and prevent further damage to heart muscle.
Then what about the other easily available tests such as ECHO cardiography and an exercise ECG? Among these two the former is used in the acute stage since it is risky to subject a patient with a heart attack to an exercise test.
Prevention of a heart attack in a patient with diabetes
Identification of those patients, who are at high risk, are of crucial importance. In a developing country such as Sri Lanka it would be very cost effective in meeting the challenge of a later heart attack, for which the treatment could be expensive. Sometimes such conditions are fatal. In this respect it should be remembered that the risk factors for heart attacks enumerated above such as high blood pressure, high cholesterol and the presence of protein in the urine too should be corrected.
Other tests that are done to decide on high risk patients consist of imaging techniques such as CT Angiography and Conventional Angiography. The latter however is considered to be the ‘Gold Standard’ in identifying high risk patients.
Prevention of diabetes
Of course prevention of DHD consists first of all preventing diabetes at any level. There are four strategies for prevention.
1.Primary prevention-That is the prevention of diabetes in the first place by adopting certain lifestyle measures such as diet, exercise and stress relief methods such as meditation.
2.Secondary prevention- Is the prevention of organ complications in those who have already developed diabetes.This again consists of adopting proper lifestyle factors mentioned above as well as attending to other risk factors such as high blood pressure and blood sugar.
3.Tertiary prevention- Is lessening of further organ damage in those who already have organs that are affected.
4.Primordial prevention-There is new evidence that certain people are programmed to survive in an adverse environment such as scarcity of food in environment when they are born underweight. If they are over fed in later life to bring them upto their ‘normal weight’ called ‘catch up’ growth. This would later lead to diabetes in this baby when it is older.
Screening of undiagnosed diabetes
It has been stated that for every patient with diabetes there is another one who remains undiagnosed and therefore could be subjected to heart attacks without even knowing that they ever had diabetes. That is why it is very important to identify these apparently unaffected patients.This is called screening and there are three types:
1.Universal screening-This involves screening of the whole population for diabetes which is obviously impracticable even in more developed countries.
2.Opportunistic screening- Screening that is carried out when the opportunity arises such as when they present to a medical officer for another illness.
3.High risk screening- This is the most important of the screening methods where those who are at a high risk of developing diabetes are identified by a simple blood test. These high risk patients consist of the following; those with a family history of diabetes, those with high blood pressure and high cholesterol levels and those indulging in sedentary occupations.
Screening for ‘prediabetes’
This is a recently identified concept and is diagnosed when the fasting blood sugar is between 100mg/dl and 125 mg/dl. Diabetes is of course diagnosed when the blood sugar is more than 126mg/dl.The importance of identifying this entity arises from the fact that it not only leads to overt diabetes later if not properly handled and equally important is that these patients too could sustain complications such as a heart attack or stroke. (The writer is a Retired Professor of Medicine and also served at the Faculty of Medicine, Peradeniya apart from being the Managing Director of the Kandy Diabetes Centre)
22 Dec 2024 3 hours ago
22 Dec 2024 3 hours ago
22 Dec 2024 6 hours ago
22 Dec 2024 6 hours ago
22 Dec 2024 6 hours ago





