20 Oct 2020 - {{hitsCtrl.values.hits}}
 Ensuring trust, confidence and cooperation from the general public is the key for successful control of the current situation
Ensuring trust, confidence and cooperation from the general public is the key for successful control of the current situation
 As the debate continues on whether Sri Lanka is in Stage 4 of COVID transmission or not, medical experts and health authorities also seem to be in a tug-of-war. While their opinions are divided, it is ultimately the people who will experience the brunt of this situation. It could be that the country cannot go into another indefinite curfew period due to socioeconomic reasons, but all lives and their health matter in this situation. Therefore, while authorities urge the public to place trust in the health system, medical experts request authorities to do ‘more’ to build trust among people.
As the debate continues on whether Sri Lanka is in Stage 4 of COVID transmission or not, medical experts and health authorities also seem to be in a tug-of-war. While their opinions are divided, it is ultimately the people who will experience the brunt of this situation. It could be that the country cannot go into another indefinite curfew period due to socioeconomic reasons, but all lives and their health matter in this situation. Therefore, while authorities urge the public to place trust in the health system, medical experts request authorities to do ‘more’ to build trust among people.
Time to admit that there’s a community transmission
 “We need to get over the ‘cluster’ mentality,” warned Dr. Ruvaiz Haniffa, Consultant family physician and head of the Family Medicine Unit at Colombo University. “We in Sri Lanka, with our solid foundation in public health should first admit that there’s a community transmission (Stage 4) based on evidence. Still they haven’t traced the index case. How can there be many positive cases detected in a single day? There are psychosocial issues related to COVID-19, but we don’t talk about them. Patients experience anxiety because they are uncertain about another lockdown. There are people who are unemployed due to the pandemic. There has to be a balance between life and livelihoods.” said Dr.Haniffa.
“We need to get over the ‘cluster’ mentality,” warned Dr. Ruvaiz Haniffa, Consultant family physician and head of the Family Medicine Unit at Colombo University. “We in Sri Lanka, with our solid foundation in public health should first admit that there’s a community transmission (Stage 4) based on evidence. Still they haven’t traced the index case. How can there be many positive cases detected in a single day? There are psychosocial issues related to COVID-19, but we don’t talk about them. Patients experience anxiety because they are uncertain about another lockdown. There are people who are unemployed due to the pandemic. There has to be a balance between life and livelihoods.” said Dr.Haniffa.
He further said that people should place their trust in the public health system. “So once we get over the ‘cluster’ mentality as a nation and take the public in to our confidence and empower them to trust the public health system and other genuine health experts, the solution to mitigation of COVID community spread will emerge by a collaborative effort between people and health experts. This is in fact, the need of the hour,” he added.
Community spread- WHO classification not a helpful guide : Dr. Rannan-Eliya
 International medical researcher and Executive Director at Institute of Health Policy Dr. Ravindra Rannan-Eliya says that the spread was presumably happening during September and even earlier.
International medical researcher and Executive Director at Institute of Health Policy Dr. Ravindra Rannan-Eliya says that the spread was presumably happening during September and even earlier.
QHealth officials are repeatedly denying that a community spread has begun. They claim that the WHO definition doesn’t fit. What are your observations about this new situation?
We still don’t know when the Minuwangoda cluster started. I think officials are hiding behind a totemistic regurgitation of definitions, and a failure both to communicate clearly and to acknowledge the seriousness of the situation. The public understands community spread to mean what common sense would suggest, i.e., that the spread of the virus is occurring between unrelated households and individuals who have little connection with each other. We should fear this as it substantially increases the risk that the outbreak will spiral out of control. This spread is clearly happening.
However, ‘community spread’ as defined by WHO and other health agencies for infectious diseases does not have this common sense meaning. WHO and others, including the US CDC, narrowly use this term to mean cases where the transmission link to other cases cannot be traced.
The problem with this WHO definition is that it does not imply anything about how intense or widespread the epidemic is. For example Country A might have 1 new case a day without any increase over time, but not be able to identify the origins of these cases because its contact tracing is inefficient or not happening. Country B on the other hand might be having 10 new cases a day, with this gradually increasing over time to 100 new cases/day, but be able to trace the origins of each case through contact tracing. According to the WHO, Country A would have community transmission, but not country B.
Personally, I think we need to get away from this narrow WHO/CDC perspective. COVID-19 is critically different from many other viruses that we have traditionally dealt with. It is much more serious than flu, and unlike Ebola or SARS or flu, the virus is frequently transmitted by people who are not sick. When I look at the countries that have succeeded in preventing a second wave, they don’t fixate on this WHO classification. Instead they all focus on a clear distinction between “imported” cases and “local” cases, with the WHO criterion of whether the transmission chain being of secondary importance. The first goal in these countries is not to stop “community transmission” as defined by WHO, but to minimise and stop local transmission. We need to make a similar shift in mindset.
QDo you think increasing PCR capacity alone would help mitigate this situation?
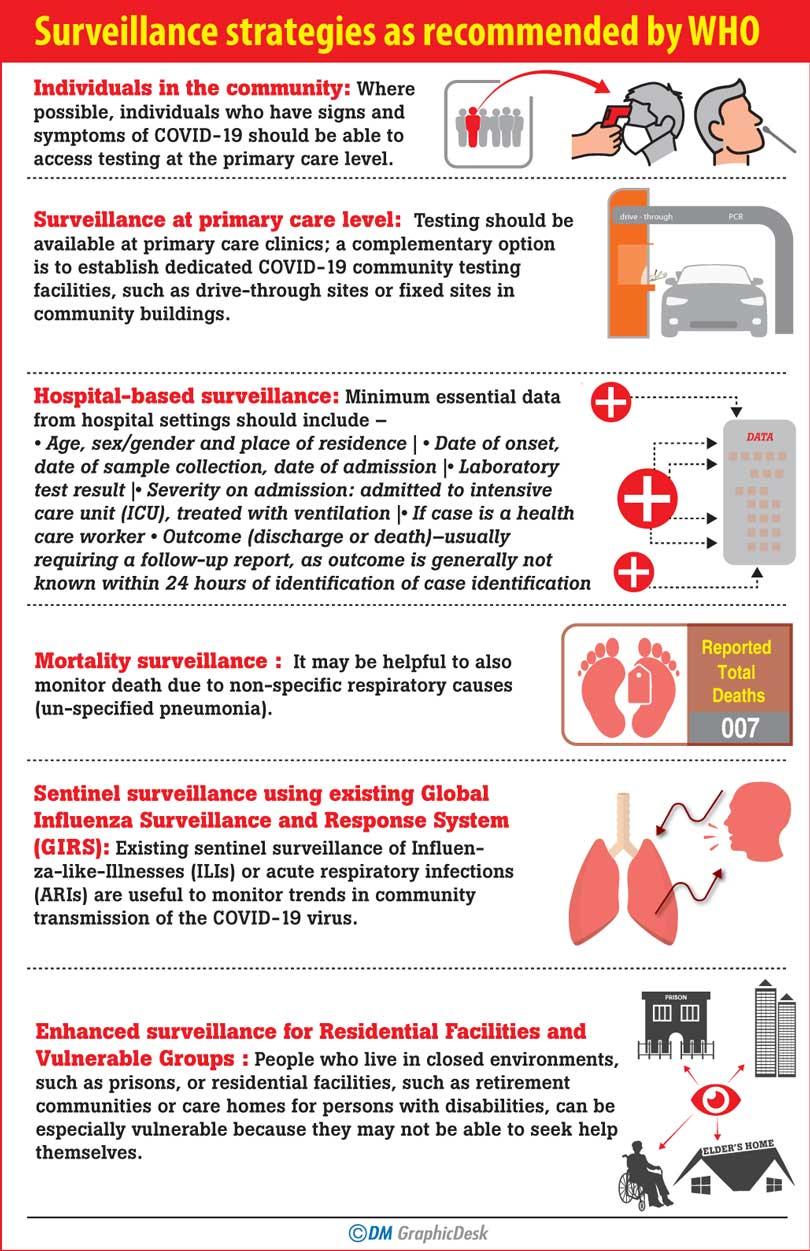
If we are to prevent a second wave as a few countries have managed to do, we need to follow their examples and not robotically follow WHO terminology. All these countries rely on vastly increased PCR testing, in addition to contact tracing and isolation. Testing not only of cases and their contacts, but also people in the community who are suffering from respiratory symptoms or fever. So yes, we need to vastly increase our PCR capacity. This part is missing and needs to supplement the contact tracing and isolation. I hope that the President and PM understand this and push MOH to take urgent action to increase our testing capacity and also start systematic testing of people with symptoms in the community. Otherwise there is a significant risk that in time to come we will face a large second wave, and the public will unfairly blame the President for the failures of the health authorities.
QCan all positive cases be linked to one cluster ?
Our contact tracing is good, so it may be possible in time, but, the larger the outbreak the greater the risk that we will find cases where we cannot find a link, plus we only trace the contacts after they have already infected others. The effectiveness of the tracing is not the only measure we need to look at. We also need to worry about the size of the outbreak itself and how long it lasts.
QIf we go to Stage 4 …
My professional judgment based on the scientific evidence is that the WHO classification is not a helpful guide to action in the case of COVID-19. So I do not use this staging to assess the situation.
Right now, my concerns are two-fold:
1) Despite largely crushing the virus by May, we keep on having these large outbreaks. These are much bigger than the ones that have happened in China, Vietnam, New Zealand, Taiwan, Bhutan and Australia (excluding Victoria). We are taking too long to detect these because our testing strategy is flawed. We need to fix this to reduce the risk of large outbreaks to near zero.
2) The risks with these large outbreaks are several fold. First, they may become so large that they out-run our ability to contact trace and isolate effectively, creating the risk that the virus gets out of control and we end up like much of the rest of the world. Second, the wide spread of the current cluster, even if all cases can be linked, is seriously inconveniencing the public, businesses and school children, as well as creating fear. Increasingly thousands of innocent people are being caught up as contacts and being suddenly quarantined. This may be immediately necessary, but the need could have been avoided.
QIs it wise to continue operations without going into a lockdown?
This is a difficult question to answer. There is growing global evidence which suggest that lockdowns haven’t always been effective in slowing down the virus. One can think of India and many other countries as examples. They have worked in a few instances, for example in parts of Europe and in Wuhan (China), but in far more cases they have not. Most of the successful countries so far have anyway not relied on lockdowns as a control measure - this includes most parts of China outside Wuhan, Vietnam, Singapore, most of Australia, Taiwan, Korea, etc.
At this stage, a ramped up and smart testing strategy might be sufficient to control this in combination with the current contact tracing and isolation efforts. However, if all else fails, then draconian lockdowns might be the only solution to allow our testing, tracing and isolation efforts to get things under control. We desperately need to ramp up testing capacity now and over the longer term to avoid having to make that choice.
Cannot define current situation as community transmission yet
When asked about the possibility of a community spread, President of Sri Lanka Medical Association, Prof. Indika Karunathilake said that the priority at the moment is to break the chain of transmission. “There’s a technical difference between patients being found from the community and a community spread of an epidemic. The community spread is a serious situation where large numbers of patients who cannot be traced to an index case are found and the epidemic has gone out of control. So we cannot define the current situation as community transmission as of yet. However, we are probably on the verge of a community transmission unless urgent and effective measures are taken.” said Prof. Karunathilake.

So we cannot define the current situation as community transmission as of yet. However, we are probably on the verge of a community transmission unless urgent and effective measures are taken
Prof. Indika Karunathilake
He further said that the gazette on COVID preventive measures that was issued recently should be strictly implemented at all levels. “Still there is no need for an island-wide lockdown. Mobility in seriously affected areas needs to be restricted while maintaining economic activities, essential services and supply chains. With many positive cases being detected, it may not be possible for health system to manage all asymptotic cases within hospitals and there is a need to identify separate facilities to isolate and monitor them. There has to be a good collaboration between different sectors including health, security forces and law enforcement. Ensuring trust, confidence and cooperation from the general public is the key for successful control of the current situation.” said Prof. Karunathilake.
Vulnerable period
Commenting on the topic, Government Medical Officers Association Secretary Dr. Haritha Aluthge said that the current situation is different to what happened in March. “Patients were reported in different durations, but today many are being reported in a single day. In order to analyze if we are in a community transmission period or not, we need proper data as we cannot analyse it only using media reports. Therefore the Epidemiology Unit should share this data with the rest of its stakeholders.” said Dr. Aluthge.
He added that although the Army Commander and Police Media Spokesman said that we are not yet in community transmission and that all cases are linked to the Minuwangoda cluster but there is no official statement as yet. “Different factions are giving different statements and this doesn’t look good in this situation. Although it is too early to predict if we are in Stage 4 of COVID transmission, this is a very vulnerable period and the impending threat to shift to a community transmission is at its highest.” he warned.
“In April we presented an exit strategy and according to that we suggested zonal lockdowns in high risk zones,” he continued. “This is because it is impossible to go in for an island-wide curfew period again. Out of the 340 MOH areas, 30 have been identified as high risk areas. These areas could be locked down to minimise the risk. We also saw the emergence of sub clusters, but it would be only in two weeks time that we could confirm if these are isolated incidents or not. This is because the incubation period is two weeks. Authorities such as the Health Promotion Bureau should consider promoting risk communication strategies when dealing with the public. It is only then that people would realise the gravity of the situation.” he said.

Although it is too early to predict if we are in Stage 4 of COVID transmission, this is a very vulnerable period and the impending threat to shift to a community transmission is at its highest
Dr. Haritha Aluthge
Dr. Aluthge further said that while adhering to routine health habits it is also important to improve respiratory etiquette to contain further spread of the virus in addition to a behavioural change. Commenting on identifying the index case, he said that it is crucial that the Police and Armed forces speed up investigations and reveal from where this new outbreak emerged.
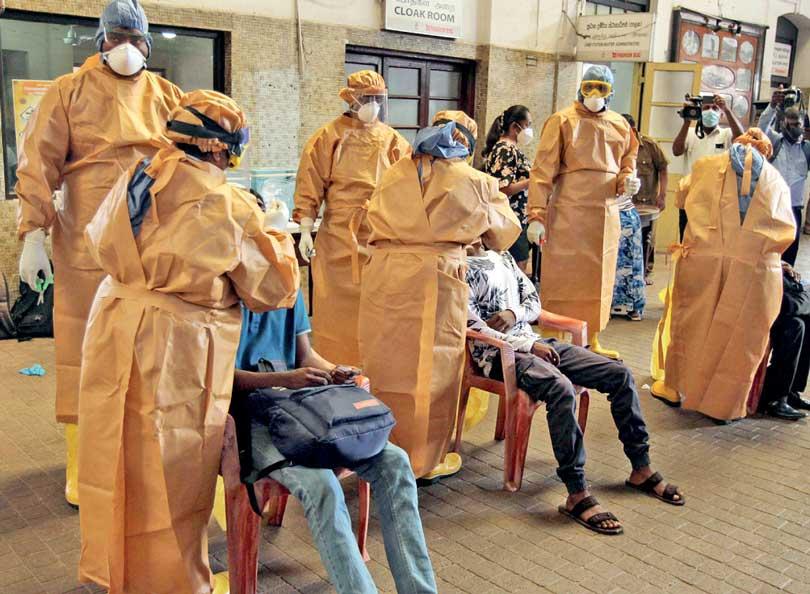
pix by pradeep dilrukshana
 Sri Lanka also needs to worry about the size of the outbreak itself and how long it lasts
Sri Lanka also needs to worry about the size of the outbreak itself and how long it lasts
27 Nov 2024 2 hours ago
27 Nov 2024 3 hours ago
27 Nov 2024 3 hours ago
27 Nov 2024 4 hours ago
27 Nov 2024 4 hours ago