20 Jan 2021 - {{hitsCtrl.values.hits}}
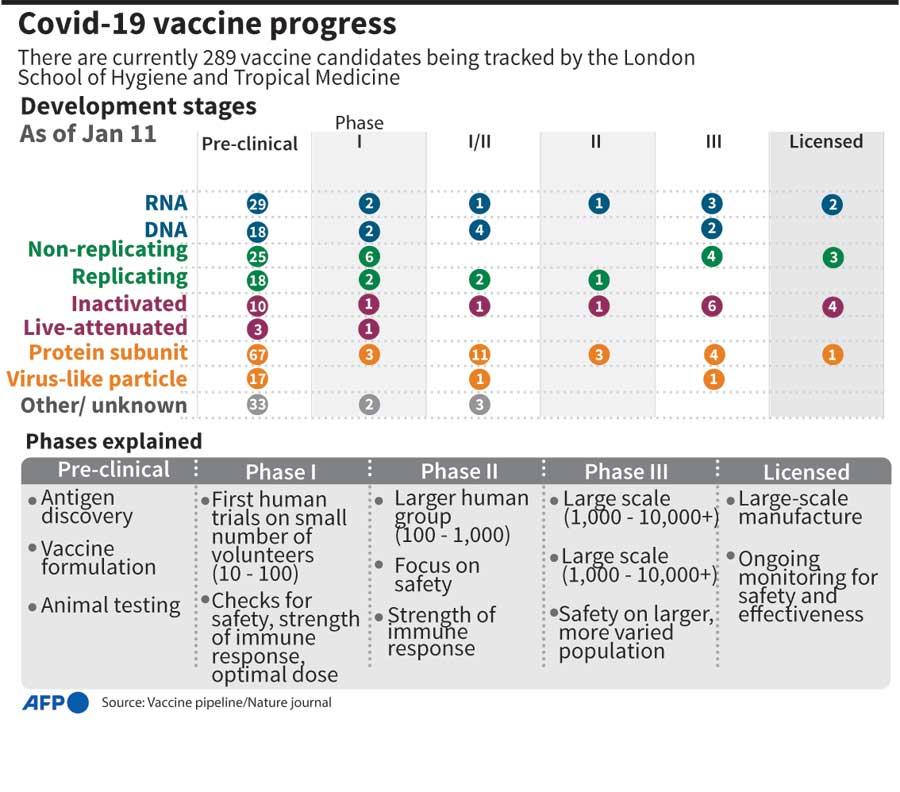
Sri Lanka is faced with two COVID-19 related medical issues. The first is, which vaccine should we give our  population, i.e., US, UK, Russian, Chinese or Indian? International safety approvals, costs, foreign assistance and logistics of distribution and availability of cold chains are the key factors that will be considered in deciding the most appropriate vaccine for Sri Lankans. Let’s leave that to the WHO, Ministry of Health, Medical Trade Unions et al., to grapple this problem. However, once Sri Lanka is assured of some vaccine doses, a second more important issue emerges: Who should get it first?
population, i.e., US, UK, Russian, Chinese or Indian? International safety approvals, costs, foreign assistance and logistics of distribution and availability of cold chains are the key factors that will be considered in deciding the most appropriate vaccine for Sri Lankans. Let’s leave that to the WHO, Ministry of Health, Medical Trade Unions et al., to grapple this problem. However, once Sri Lanka is assured of some vaccine doses, a second more important issue emerges: Who should get it first?
The obvious and least political choice is to say that the front-line health workers should get it first. Then, who will be the next? The Security people, Grama Niladharis, and other field level Civil Servants, Politicians, Heads of Departments and Ministries or, sections of General Public who are the most vulnerable to the disease?
It will be naïve to think that Front line Health Workers, some government officials, politicians will not get it first, and we will have no control over it. The socially sensitive issues will arise after this. Who in the general public should get it first? If you take a survey, most citizens will say children first and pregnant women next. However, the tendency on many Western counties is to pick older age groups like those in their 80s and 70s first who will also be on treatment for hypertension cardiac disease, cancer, diabetes and chronic lung and renal disease. The logic that prevails in such Western countries is rather straight forward: prevention of old people getting COVID-19 as they are more likely to die as the viral infection may aggravate the existing disease conditions. The data they have supports this logic and the subsequent action. In Sri Lanka too, out of over 250 deaths, most of them had underlying diseases and were in the range 70 years by age. Even in this case, the part of the argument is that the older one is, it is likely that he or she has underlying diseases, which may be adversely affected with COVID-19 infection. In the meantime, we have heard of reports of older people who are over 90 or 100 years of age escaping the wrath of COVID-19. So, as the center of this logic, it the possibility of death or mortality that has received the attention of policy makers. In Sri Lanka however, the mortality rate is significantly less compared to the West and that leaves us with the question whether we should just blindly follow the logic used in the West to select segments of the population to receive priority in giving the vaccination against COVID-19.
On the contrary, shouldn’t we be asking who are the people most likely to get COVID-19, i.e., morbidity, rather than who are more likely to die (mortality) because of the deadly virus. The distinction between morbidity and mortality is the most basic concept used by Epidemiologists and here we argue that we make optimal use of such scientific notions to clarify our thoughts, prior to policy making.
The “Epidemiologic Gaze” of the Medical, Security and Political people in Sri Lanka shifts between two poles: Cluster vs. Community Spread. Just like them, we too cannot be definitive as the information provided from the government controlled COVID-19-programme is not easily available to make wise choices. We have been told that there are two large clusters and a several sub clusters of COVID-19 victims. On the other hand, sporadic cases of patients are detected for whom a clear chain of contact with a previously known patient may not have been found. The relationship between the two Epidemiological gazes is that in the Cluster, COVID-19 epidemic starts with a patient who spreads it to a small cluster like his family or the workplace which will be contained with rapid testing followed by isolation and curative care.
Such clusters often have a life span and can be contained with vigorous testing, isolation of contacts and treatment of positives. When victim of clusters gives the disease to unknown people, when the contacts cannot be found for testing purposes, the dreaded Community Spread commences with more and more unknown people, who are difficult to trace, get infected and starts spreading the disease, unknowingly. This will result in a national level epidemic which the Ministry of Health trying hard to contain with their limited resources.
Information made available will not make us definitive regarding the Epidemiological Gaze. If there is community spread, like in the West and in other countries where large segments of the population are affected, the old, the ill are obviously vulnerable to COVID-19 with the possible consequence of death. In such a scenario giving the vaccine to such segments of population such as the aged, diabetics, heart patients and those who in homes is logical and can be justified.
On the other hand, if Sri Lanka’s Epidemiological Gaze is more towards clusters, big or small, one could not just go by the Western approaches of COVID-19 vaccine dispensing and instead must look for more targeted approaches that will prevent further morbidity, instead of mortality. As mentioned before, if the mortality rates are low as the government claims, such a deviation in the approach could be morally justified.
Let us now take a deeper look into the “Clusters”. Ministry of Health claims that Sri Lanka has two or three very large clusters and a few sub clusters which are connected to the large clusters. Minuwangoda Cluster and the Peliyagoda Cluster are two of them. In such clusters there are thousands of COVID-19 positives that have been detected and treated. In addition, Sri Lanka had large captive samples such as those of the Navy and workers of Garment Factories. Unfortunately, not much research, either sociological or medical, have been performed on such clusters and information or data available on such clusters is therefore scanty.
It is unfortunate that very little research has gone into the ongoing COVID-19 epidemic to make information available to the policy makers to make evidence-based decisions. However, it is obvious that certain behaviours of groups of people have made the spreading of the disease faster. What this shows is that the spread of the disease from person to person or from groups of persons to others is mostly social. If sociological inquiry has gone into such cluster making phenomena, unique social networks based on common behaviours could have been identified.
Whether such information is available to the Ministry of Health or the Presidents Task Force is not immediately evident. However, the use of secret services to tract the contacts obviously shows that such networks based on specific behaviours existed at least among the Navy personal, Garment Workers and Fish vendors at Peliyagoda etc. Given this experience, it will be easy to postulate social networks through which transmission takes place exists and are active even now. Recording such networks is still an important activity to generated valid data to be made available to policy makers. It appears at times that such data have been kept confidential for fear of social and commercial negative impacts.
However, careful examination into the process of COVID-19 spread may indicate that there are other networks operating even now or could be operative in the future. Some of them could be vegetable and fish vendors, three-wheel drivers, bus drivers and conductors, spa girls, large labour force of plantation workers working in Colombo and Muslim traders. One key feature common to all of them is their mobility that has been associated with their living- a key factor in COVID-19 transmissions, especially with the presence of asymptomatic carriers. Given this, if the Ministry of Health and Presidents Task Force is seriously bent on curbing morbidity instead of possible mortalities, members of such social networks should receive the priority attention in dispensing the COVID-19 vaccine.
In summing up, what has been attempted here is to provide an alternative moral argument to what is likely to be the policy for distribution of COVID-19 vaccine in Sri Lanka. The argument here is controlling mortality to control the spread of the disease instead of attempts to minimize the deaths among old people which may have minimal effects on controlling the transmission. This approach will also benefit to the welfare of large numbers of Sri Lankans who contribute to the economy. Just like for all other vaccinations, it is argued that the Utilitarian Ethics which profess maximum benefit to the maximum number should prevail even with regard to COVID-19 vaccines.
30 Nov 2024 56 minute ago
29 Nov 2024 29 Nov 2024
29 Nov 2024 29 Nov 2024
29 Nov 2024 29 Nov 2024
29 Nov 2024 29 Nov 2024





